Following on from Mr Adrian Lower's excellent article providing an overview of uterine fibroids he has provided an indepth article on the investigations and diagnosis of this condition. This will be of help to any woman who thinks she may be suffering from fibroids and would like to know what the tests will involve.
Diagnosing Uterine Fibroids - Contents
- Introduction to fibroid diagnostics
- Transvaginal ultrasound scan for fibroids
- Saline Sonography for fibroids
- Magnetic Resonance Imaging (MRI) for fibroids
- Virtual Hysteroscopy
- Diagnostic Surgery
- Diagnostic Hysteroscopy
- Diagnostic Laparoscopy
- Summary
Introduction to Fibroid Diagnostics
The first article in this three-article series presented what fibroids are, the different types and some of the problems they cause. However, symptoms attributable to uterine fibroids can also be caused by a number of other conditions, notably ovarian cysts, endometriosis and pelvic infection. As such, it is particularly important that the most appropriate investigative technique is used to determine an accurate diagnosis and subsequent options for treatment.
In this article we look at the investigation techniques used to establish a diagnosis of uterine fibroids and to help to determine the best course of management. The final article in the series describes the common treatments for fibroids, what is involved for each and the risks and potential complications. Together, these articles put you in a position to take an active role in working with your doctor to determine what will suit you best.
Transvaginal ultrasound scan
Most gynaecologists who deal regularly with conditions including fibroids, ovarian cysts, endometriosis and pelvic infection will have immediate access to an ultrasound scanner as transvaginal ultrasonography is the first-line investigation of choice. I prefer to perform these scans myself as a great deal more information is obtained from the real-time assessment of fibroids and their relation to the cavity of the uterus than can be inferred from a report prepared by a third party.
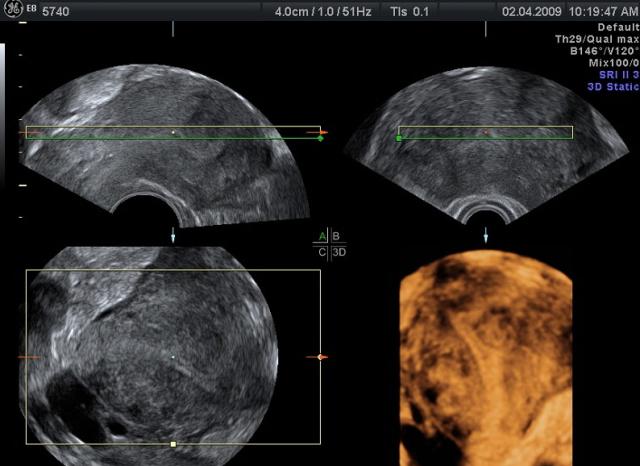
Transvaginal ultrasonography is a painless examination which uses high frequency sound waves to build up a picture of the anatomy on a video screen. The best scanners can produce images of surprisingly good resolution and clarity. In addition to the standard two-dimensional black and white images, many can obtain 3D images to more clearly define abnormalities and can also assess the blood flow to the pelvic organs and this is important.
For gynaecological conditions the best information is obtained using a transvaginal rather than abdominal probe. The ultrasound transducer is mounted on the end of a probe, no larger than your index finger, which is introduced into the vagina. This enables a higher frequency mode to be employed which improves the image resolution as the scanner is much closer to the organs of interest. Use of the transvaginal probe also means that your bladder does not need to be uncomfortably full, and better images are obtained if you empty your bladder immediately before such an examination. The examination will only take a few minutes to perform and the results are given to you at the time of the examination. The person performing the scan can show you the pictures at the time of the scan, but it does take some practice to interpret the images so the pictures may not be entirely clear to you.
Transvaginal ultrasonography alone is usually good enough to enable a clear diagnosis to be made, however, there are occasions when more information is required to be able to plan the subsequent management. Please find further information on the recommended diagnostic methods below.
Saline Sonography
This investigation is particularly useful for identifying the extent to which submucous fibroids extend into the cavity of the uterus. It is also sometimes called ‘saline infusion sonography’ or ‘sonohysterography’.

The cavity of the uterus is a potential space and although it grows to accommodate a 7lb baby during pregnancy, in the non-pregnant state the front wall lies in direct contact with the back wall. This can obscure the relationship of some fibroids to the cavity and clearer images are obtained when a small quantity of physiological saline is introduced into the womb to distend it. The fluid is introduced using a fine plastic tube through the cervix. It is no more uncomfortable than having a smear test and can be done in the practice. Fluid conducts sound waves extremely well and enhances the image of the endometrium (lining of the womb) because it creates a clear black space caused by an absence of echoes into which the ‘echo-dense’ fibroids can be seen to protrude.
Magnetic Resonance Imaging (MRI)
When fibroids are particularly large or numerous ultrasonography becomes more difficult to interpret as the sound waves only travel around 10cm through the body. In such cases more informative results can be obtained using Magnetic Resonance Imaging (MRI).
MRI is a modern imaging technique which uses the magnetic field produced by the individual molecules of which our tissues are composed to allow us to obtain very clear images showing the different structures of tissue. This is an excellent means of highlighting the size and site of fibroids and also in distinguishing between fibroids and other conditions.
MRI is a painless examination, but some scanners can cause feelings of claustrophobia. The scanners are also rather noisy. You will be required to lie still on a fairly hard platform which slides into a large cylindrical magnet and an array of sensors which whirr and click whilst the image is being acquired over a period of twenty to thirty minutes depending on the clarity of the images obtained.
New scanners have been developed called open field magnets which are less claustrophobic. The images are not always of the same quality, or as easy to interpret, but technology is changing and improving all the time. If you are concerned about claustrophobia, you may want to ask your doctor whether an open field magnet will provide an adequate quality image.
MRI images of patient before and after open myomectomy
Virtual Hysteroscopy
This is a new imaging technique using the same technology as virtual colonoscopy or CT colonography. In the case of virtual hysteroscopy, carbon dioxide is gently introduced into the womb through the cervix using a small plastic tube. This distends and separates the walls of the womb in the same way that saline is used in saline sonography.

An advanced x-ray examination called a CT (computerised tomography) scan is then performed. This produces a number of 2D “image slices” through the body, each a fraction of a millimetre apart. These images are then processed through a computer to produce a 3D reconstruction of the uterus which allows us to accurately assess the size and impact of fibroids on the cavity of the uterus (womb).
Although virtual hysteroscopy is a new technique, it is safe and offers what promises to be a highly useful alternative to saline sonography and diagnostic hysteroscopy (see below). However it is still under evaluation. The amount of radiation you are exposed to is low (although up to 100 times more than from a mammogram) but the excess risk of radiation-related cancer development as a result of this examination is less than 1 in 10,000.
Diagnostic Surgery
Where possible we try to avoid performing diagnostic surgery alone. Instead, a “See & Treat” policy is preferable as imaging will provide a pretty good idea of what we are likely to encounter. Occasionally, however, this is not possible and a diagnostic hysyteroscopy and sometimes a diagnostic laparoscopy are recommended. In addition, we sometimes recommend a diagnostic hysteroscopy after a myomectomy, particularly if the cavity has been breached or appears unusually distorted when viewed using other imaging modalities.
Diagnostic Hysteroscopy
This is performed using a fine telescope, 2 millimetres in diameter, which is introduced through the cervix using physiological saline or carbon dioxide to distend the cavity. A clear view of the endometrial surface of the uterus is obtained and adhesions and submucous fibroids can be identified, allowing a careful assessment to be made of any anatomical disturbance. The procedure is usually performed in an operating theatre or purpose designed outpatient procedure suite and can be done under local anaesthetic, but a general anaesthetic may also be used if you find internal examinations uncomfortable. Even if a general anaesthetic is used you will only need to be in hospital for a few hours.
Diagnostic Laparoscopy
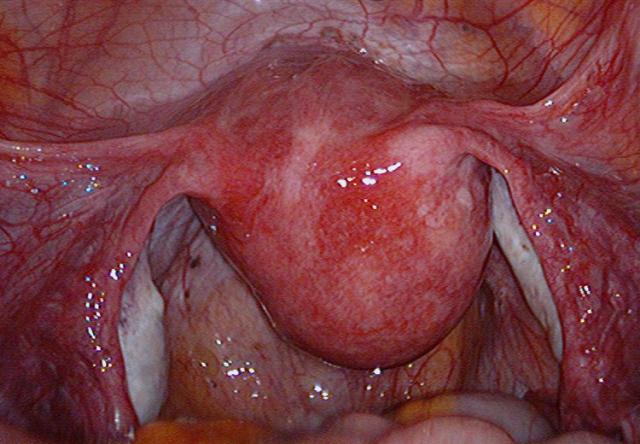
Diagnostic laparascopy, usually requires a general anaesthetic as it involves the distension of the abdominal cavity with carbon dioxide to create a space into which a small telescope can be introduced. The carbon dioxide is introduced using a small needle, 1 millimetre in diameter, inserted through the navel and this can be quite uncomfortable and cause distressing feelings of breathlessness if you are awake. There is a small risk (less than 1 in 1000 cases) that this needle could damage the bowel, blood vessels or bladder. The risk is higher where there are extensive adhesions from previous surgery or unexpected anatomical variations.
Once the abdomen is distended with carbon dioxide, a 5 millimetre port is then introduced through the navel into the space created by the introduction of the gas. A 5 millimetre telescope is passed through, from which video images of the abdominal cavity are obtained. Often a second port is introduced so that a probe can be used to move the organs around to improve the view.
Like diagnostic hysteroscopy, diagnostic laparoscopy is performed in an operating theatre and you will usually be allowed home a couple of hours after the procedure, once the effects of the anaesthetic have worn off, unless you have an adverse reaction to the anaesthetic. Modern anaesthetic techniques are safe and usually well tolerated and so adverse reactions are extremely rare. Sometimes there can be inherited sensitivities to some sorts of anaesthetics which you will almost certainly be aware of if your family is affected. It is important that you tell your anaesthetist about this if anyone in your family has had a problem in the past.
Summary
Using the investigations described above, your gynaecologist will be well placed to discuss the size, site and number of fibroids in your uterus, their relation to the cavity of the uterus and depending on your symptoms and desire for a family, he or she will be in an excellent position to assist you in making an appropriate decision regarding management. The methods of managing fibroids are described in the next article.



