Explaining the symptoms and types of hydrocephalus, a rare paediatric condition. This article will be of help to any parent or carer who would like to know what treatment options exist for children suffering from hydrocephalus.
Contents
- Introduction
- Definition
- Types of hydrocephalus
- Symptoms of hydrocephalus
- Treatment of hydrocephalus
- Endoscopic Third Ventriculostomy
- Removal of the tumour
- Which procedure?
- Summary
Introduction
Though brain tumours in children are rare their consequences can be devastating. Hydrocephalus when present in children with brain tumours will require surveillance and treatment long after the brain tumour has been successfully cured. This article attempts to describe hydrocephalus and its treatment in children who have brain tumours.
Definition
Hydrocephalus is a condition whereby there is an imbalance between the production and reabsorption of cerebrospinal fluid (CSF) within the brain. CSF is a clear colourless fluid that is produced and contained within chambers lying inside the brain (known as cerebral ventricles) and also within the subarachnoid and subdural spaces that surround the brain and spinal cord. Thus the brain and spine float in a ‘bath’ of CSF.
The ventricular system consists of four chambers; two lateral ventricles each of which connects through a small opening known as the Foramen of Monro into the midline third ventricle, which itself drains into the fourth ventricle through a narrow opening (known as the Aqueduct of Sylvius). The fourth ventricle has three exits that allow CSF to drain out into the subarachnoid space. Each of these four chambers are connected such that the CSF is able to flow from one end to the other before exiting the last chamber and flowing around the surface of the brain and spinal cord before being reabsorbed via microscopic channels (arachnoid granulations) into the circulation. Any process that physically blocks the movement of CSF from one chamber to another or prevents CSF from being reabsorbed into the circulation can result in an abnormal accumulation of CSF. Hydrocephalus may present with a progressive rise in the intracranial pressure and, if not treated, has the potential to cause severe brain damage or even death.
Types of hydrocephalus
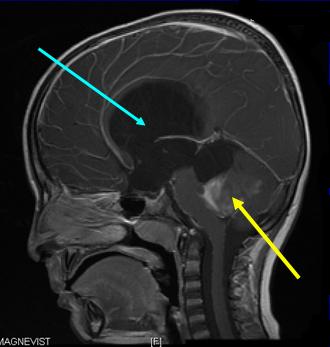
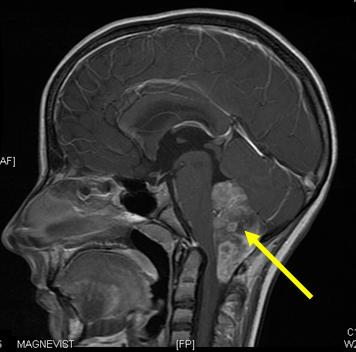
Obstructive hydrocephalus is caused by a physical obstruction to the normal flow of CSF from one chamber to another. This is most commonly due to either a tumour growing within and occluding (closing off) one of the cerebral ventricles or growing in the brain adjacent to the ventricle, which compresses, obstructs or distorts the ventricle. CSF cannot, therefore, flow past the tumour and the cerebral ventricle(s) expand(s) above the blockage. The characteristic feature of this type of hydrocephalus on scans is the presence of expanded cerebral ventricles above the blockage and normal sized ventricles below the blockage.
If untreated, the child will develop raised intracranial pressure, and, at this point, it will become necessary to undertake emergency surgery to relieve the pressure. Treatment may be required to directly drain the fluid, remove the tumour or a combination of both.
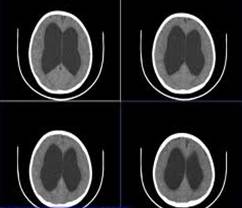
In contrast, communicating hydrocephalus can be caused by any pathological process that blocks the microscopic channels through which CSF is reabsorbed back into the bloodstream. Common causes of this type of hydrocephalus are bleeding into the cerebral ventricles, infections such as ventriculitis or meningitis, or the presence of tumour/tumour cells within the ventricular system. The characteristic feature of this type of hydrocephalus on scans, is uniform enlargement of all of the cerebral ventricles. Again, if untreated the child will develop raised intracranial pressure and surgery will be required to divert the flow of CSF to another body cavity (such as peritoneum, pleural cavity) where it can be reabsorbed.
Tumour associated hydrocephalus is a frequent manifestation of a number of different childhood brain tumours as many of these tumours are located within or adjacent to the cerebral ventricles. Its management can be extremely complex and can be as challenging as managing the tumour itself. The ventricular system may be blocked at any point by a tumour, though there are certain consistent locations where this occurs in childhood.
It is easiest to consider the management of tumour associated hydrocephalus (TAH) by looking at each different type of childhood tumour and where it obstructs the ventricular system.
| Location | Tumour Types | Ventricular Obstruction |
|---|---|---|
| Posterior fossa: cerebellum brainstem fourth ventricle |
Medulloblastoma Ependymoma Juvenile pilocytic astrocytoma Choroid plexus tumours |
Fourth ventricle |
| Suprasellar | Craniopharyngioma Germ cell tumours Hypothalamic-chiasmatic tumours |
Third ventricle |
| Pineal | Pineoblastomas Astrocytomas Germ cell tumours |
Aqueduct |
| Tectal plate | Astrocytomas | Aqueduct |
| Third ventricular tumours | Astrocytomas | Third ventricle |
| Lateral ventricle | Segca | Foramen of monro |
The most common childhood tumours causing hydrocephalus are found in either the cerebellum or fourth ventricle and may be benign or malignant. Less common tumours may be found in the pineal region or tectal plate compressing the aqueduct, craniopharyngiomas and hypothalamic-chiasmatic gliomas which may compress the third ventricle, subependymal giant cell astrocytomas (found in tuberose sclerosis) which may block the Foramen of Monro. Tumours that have spread diffusely within the ventricles (usually malignant) may also cause a communicating hydrocephalus by blocking CSF reabsorption pathways. Benign cysts (Arachnoid Cysts) may, by their size and position within the brain, mimic tumours and physically obstruct any part of the ventricular system.
Symptoms of hydrocephalus
In neonates and small babies, recognising hydrocephalus may be difficult as some of the symptoms and signs are not uniquely specific to hydrocephalus. Of particular importance:
- Excessively large head
- Head circumference measurement that is accelerating abnormally fast
- Decreased level of consciousness
- An anterior fontanelle that is tense and bulging
- New onset squint
- ‘Sunsetting’ eyes (unable to look upwards)
Other less specific symptoms of raised intracranial pressure include poor feeding, failure to thrive, irritability and vomiting. However, they are also non-specific signs of other diseases and may therefore lead to delay in the diagnosis.
In older children who may be able to speak, there are a number of different symptoms that may be present:
- Headaches
- Vomiting
- Blurred vision
- Double vision
These are significant, and should be taken seriously. Other symptoms include slowed mentation, unsteadiness of gait or imbalance. In more advanced cases, the child may present with an impaired level of consciousness or in a coma.
On examination, the child may have papilloedema, loss of upward gaze, a sixth cranial nerve palsy (and failure of lateral gaze), truncal ataxia (unsteady or uncertain walking) or a decreased level of consciousness. The presence of any of these signs should initiate an immediate CT scan to look for hydrocephalus.
In patients who are known to have hydrocephalus, the failure of the shunt valve to refill after it is depressed is strong circumstantial evidence of shunt malfunction.
Treatment of hydrocephalus
The management of tumour associated hydrocephalus in children is controversial and can vary considerably depending on the location and type of tumour that is present. However, the absolute priority is a careful and thorough clinical assessment of the patient by the clinical team to ascertain the neurological state of the child. Following this, the child requires neuroimaging, with CT scans often being the easiest and quickest scans to undertake.
In all children with a tumour, magnetic resonance imaging (MRI) of the whole neuraxis is mandatory to determine the accurate location and extent of the tumour and the severity of the hydrocephalus.
The most critical decision for the clinician at this stage is to determine what is most symptomatic: the hydrocephalus or the tumour. Often it is the hydrocephalus that is responsible for the immediate life threatening danger to the child. Swift treatment of the hydrocephalus takes the child out of danger and allows the neurosurgical team to plan the optimal management of the tumour, and often creates a safer operation to remove the tumour. It also frequently prevents the need to immediately undertake removal of the tumour, instead allowing time for the high intracranial pressure to subside.
It is easiest to look at the treatment options by considering where the tumour is located. The most common location for childhood tumours is within the area of the brain known as the posterior fossa. This includes tumours of the cerebellum, fourth ventricle and brainstem.
For posterior fossa tumour associated hydrocephalus, there are four main strategies of management (in order of surgical difficulty):
- Insertion of an external ventricular drain (EVD)
- Insertion of a ventriculo-peritoneal shunt
- Endoscopic third ventriculostomy (ETV)
- Removal of the tumour
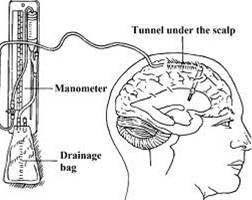
Insertion of an external ventricular drain is a neurosurgical procedure that all neurosurgeons are competent to perform. It is one of the most common procedures undertaken across all neurosurgical units and is very quick and minimally invasive. It involves making a small hole in the skull, often in the frontal region, the insertion of a fine tube into the ventricle and attachment of this tube to an external drain where the amount of CSF can be carefully controlled. In an immediate, life threatening situation it is the procedure of choice due to the speed and ease with which it can be done (even in an emergency room or paediatric intensive care unit if necessary).
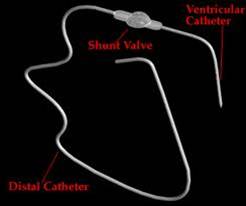
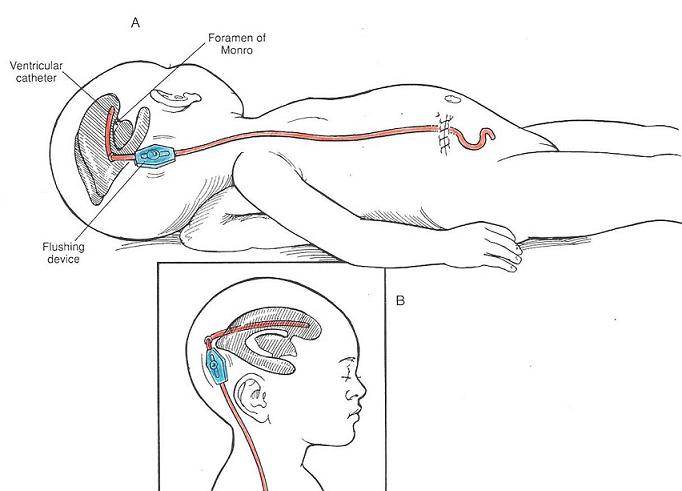 Insertion of a ventriculo-peritoneal shunt is a procedure that all paediatric and most adult neurosurgeons are technically competent to undertake, and for paediatric neurosurgeons, one which they frequently perform, often more than any other procedure. It involves making a small hole in the skull, placing a thin tube into the ventricular system, attaching this tube to one side of a small valve which controls the flow of CSF and finally, attaching the other end of the valve to a piece of tubing that is tunnelled under the skin and through a small abdominal incision into the abdominal cavity. This allows the CSF to drain out of the head and into the abdominal cavity, where it can be reabsorbed. The amount of CSF can be slightly moderated by the type of valve inserted. It is a longer operation than placement of an external ventricular drain, and for small babies requires a specialised team to perform the procedure.
Insertion of a ventriculo-peritoneal shunt is a procedure that all paediatric and most adult neurosurgeons are technically competent to undertake, and for paediatric neurosurgeons, one which they frequently perform, often more than any other procedure. It involves making a small hole in the skull, placing a thin tube into the ventricular system, attaching this tube to one side of a small valve which controls the flow of CSF and finally, attaching the other end of the valve to a piece of tubing that is tunnelled under the skin and through a small abdominal incision into the abdominal cavity. This allows the CSF to drain out of the head and into the abdominal cavity, where it can be reabsorbed. The amount of CSF can be slightly moderated by the type of valve inserted. It is a longer operation than placement of an external ventricular drain, and for small babies requires a specialised team to perform the procedure.
Endoscopic Third Ventriculostomy
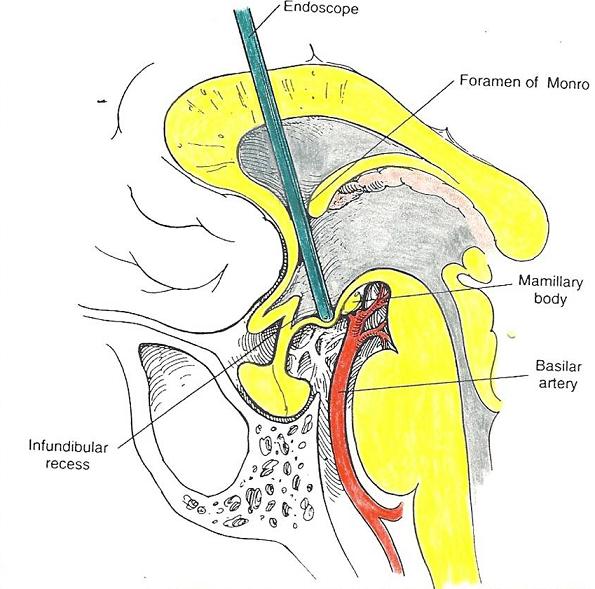 Endoscopic Third Ventriculostomy (ETV) is a highly specialised technique whereby a small, specialised neuroendoscope is passed into the ventricular system through a small hole in the skull. A hole is then made in the floor of one of the ventricles (usually the third ventricle) to allow the free flow of CSF past the point where it is blocked by the tumour.
Endoscopic Third Ventriculostomy (ETV) is a highly specialised technique whereby a small, specialised neuroendoscope is passed into the ventricular system through a small hole in the skull. A hole is then made in the floor of one of the ventricles (usually the third ventricle) to allow the free flow of CSF past the point where it is blocked by the tumour.
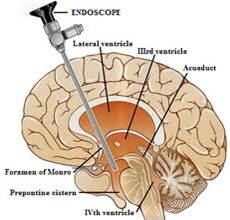
In simple terms, a short cut is made for the CSF to flow past the blockage (tumour). Because it is such a specialised technique and requires complex equipment, this is not practised by all neurosurgeons and should only be undertaken by those who regularly perform the procedure. Often at the end of the ETV a small ventricular catheter attached to a tiny button reservoir is left in place under the skin. This allows CSF to be easily sampled or withdrawn. This procedure can be performed in children of any age, is quick and minimally invasive.
Removal of the tumour
Given that it is the tumour that is causing the hydrocephalus, some neurosurgeons consider the optimal way of relieving the hydrocephalus to be removal of the tumour. This, however, is a major procedure, requires a surgeon uniquely qualified to perform this type of surgery and carries significant risks. Tumour removal is not indicated if the child is not physiologically stable or is seriously neurologically compromised by acute, decompensating hydrocephalus. Some surgeons will, at the outset of the procedure, put into place an external ventricular drain to allow for the drainage of CSF during and after the procedure before removing the tumour itself.
Which procedure?
Posterior fossa tumours
The decision about the optimal way of managing the hydrocephalus associated with posterior fossa tumours is tailored to each patient and depends on the position of the tumour within the brain, the skill of the surgeon, the equipment available, and the severity of the hydrocephalus.
In tumours of the posterior fossa, the choice is usually between either placement of an EVD or an ETV. An EVD is simple, quick and effective. It can be set up to drain CSF at a rate determined by the surgeon so as to not overdrain and risk the complications of lowering intracranial pressure too quickly. It can be left in place after the tumour has been removed. An ETV is a more complex procedure, has more serious potential risks than either an EVD or a shunt, requires the most specialised equipment, but is the most physiological means of CSF drainage. Insertion of a shunt is a permanent procedure, requiring two incisions, one in the scalp and one in the abdomen, and if the patient does not have post-operative hydrocephalus becomes unnecessary, and shunt-associated complications are common. Some surgeons prefer to proceed directly to tumour removal with placement of an EVD just before commencing tumour removal, though if the patient presents at night or on a weekend it may not be the optimal time to consider an emergency tumour operation.
There does not appear to be a consensus between the paediatric neurosurgeons worldwide as to the optimal means of controlling hydrocephalus caused by posterior fossa tumours so it is reasonable for the operating surgeon to consider any of these. EVD are associated with the lowest complication rates compared with the other drainage procedures and shunts are associated with the highest, particularly as the complications associated with shunts continue for as long as the shunt remains in place. There is evidence that children who undergo ETV prior to tumour resection may have a lower incidence of post-operative hydrocephalus than patients who have an EVD, or an EVD plus tumour resection as a single procedure.
Suprasellar region tumours
When considering tumours that occur in the suprasellar region, the treatment options are more complicated. These tumours usually cause hydrocephalus by blocking the third ventricle. In some tumours found in this area of the brain the treatment is not with surgery, but combinations of radiotherapy and chemotherapy. If surgical removal of the tumour is contemplated, such as with craniopharyngiomas and astrocytomas, then a temporary solution is preferred. In these cases, placement of an external ventricular drain is often undertaken. If the tumour has a large cystic element, an endoscopic procedure may be performed to puncture the cyst within the third ventricle to relieve the obstruction to the ventricular system, with an EVD often left in place as well.
If the tumour is a germ cell tumour (primarily treated with a combination of radio and chemotherapy, rather than surgery), a ventriculo-peritoneal shunt is the preferred option as it often takes several weeks for the tumour to shrink enough to relieve the hydrocephalus.
Pineal region tumours
There are a wide variety of different tumour types in the pineal region and most cause obstructive hydrocephalus by compressing the aqueduct of Sylvius at the back of the third ventricle. Again, there is a choice of procedures: EVD, ventriculo-peritoneal shunt, and ETV. However, using an endoscope to perform an ETV has an advantage over the other procedures. If an ETV is performed, it is often possible to obtain a biopsy of the tumour at the same time as performing the third ventriculostomy. This may prevent the need for any further surgery to identify the tumour type, and some pineal tumours (germ cell tumours) do not require surgery, but respond well to combinations of radiation and chemotherapy.
Summary
There are three main treatment options for children with hydrocephalus caused by a brain tumour, an external ventricular drain that is quick and has the lowest complication rate, an endoscopic third ventriculostomy that requires a surgeon who is specially trained and complex equipment, and a ventriculo-peritoneal shunt which is a bigger operation and is associated with the greatest number of complications. The hope, in most of these children, is that once the tumour is removed the obstructive hydrocephalus will resolve and thus not require a permanent solution (a ventriculo-peritoneal shunt).
For further information on the author of this article, Paediatric Neurosurgeon, Mr Christopher Chandler, please click here.
Associated with the nervous system and the brain.
Full medical glossary
