
Editor's comment - the details described in this news item have been widely reported and links are provided to the sources. Anyone concerned about whether vaccines are appropriate for them should seek advice from their doctor.
The Oxford Centre for Evidence Based Medicine have consistently maintained that interventions and lockdowns have made any difference to the course of the SARS-CoV- 2 pandemic. The original publications including the NEJM concluded with stating high efficacy rates for the COVID vaccines. The study conclusion stated, "A two-dose regimen of BNT162b2 conferred 95% protection against Covid-19 in persons 16 years of age or older. Safety over a median of 2 months was similar to that of other viral vaccines. (Funded by BioNTech and Pfizer)".
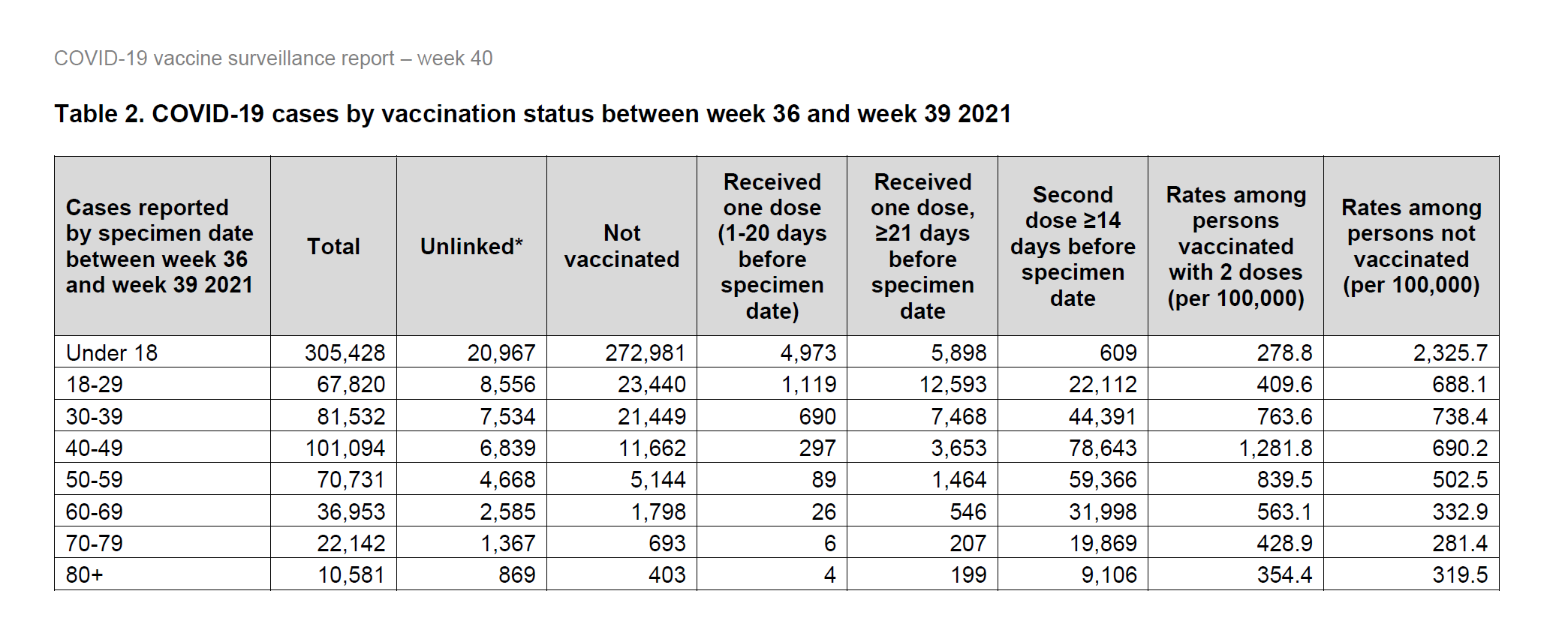
It is generally accepted that even if this was the case (and it is questionable), it certainly isn't now. Indeed, the recent official surveillance data is showing higher rates of infection in the double jabbed compared to unjabbed (see chart). Furthermore, despite lockdowns and the vaccine, for the past 15 weeks, the number of deaths in England and Wales have sadly been consistently considerably higher than for the same period last year.
The BMJ exposed a number of revelations with regard to how the clinical trials on the Pfizer vaccine were (mis) managed. Claims over "falsified data" have raised serious questions over the integrity and the regulatory oversight that allowed the approval for the launch of the Pfizer COVID mRNA vaccine.
The Oxford Centre for Evidence Based Medicine (CEBM) have now also demonstrated how measuring vaccine efficacy from population data can be misrepresented to paint different pictures. They point this out saying, "Measuring the effects of vaccines using population data is not straightforward. It can produce misleading results and inherent biases, which are difficult to spot, particularly if an important confounder such as the seasonal effect is overlooked".
The comments are a consequence of reviewing the Office for National Statistics (ONS) who published a report based on an analysis of deaths involving COVID-19 that occurred between 2 January and 2 July 2021 in England, by vaccination status.
Looking at the presentation you could conclude that there is a much larger percentage of deaths in the unvaccinated group from COVID-19 compared to the fully vaccinated group, where COVID-19 deaths appear to make up less than 1%, which the CEBM say, "is a stunning difference whichever way you look at it".
Surely such a difference is overwhelming evidence of the benefit of the COVID-19 vaccine?
no reliable evidence that the vaccines reduce all-cause mortality
Results would have been the same if treatment ineffective
However, the presentation does not take into consideration fundamental statistical factors including the effect of timing. CEBM point out, "Hence, a direct comparison of COVID-19 deaths as a percentage of all deaths is a mixture of the actual vaccine effect and the biases due to confounding by time period and COVID-19 risk. Even if the vaccine were ineffective, a comparison of two such groups confounded by time would still produce a large “effect”.
Looking at 'real world' data it is now generally known and accepted that the so-called COVID vaccines will not prevent you getting the disease, or stop you from spreading it. Boris Johnson himself has said, "I am concerned about the Delta variant being passed between those who are vaccinated and indeed those who are double vaccinated".
We are told that this is the reason for requiring more boosters, however there is major concern that this approach is not only flogging a dead horse, but carries real risk. The risk is that the mRNA vaccines are now known to cause adverse events - including stroke and heart disease. However, possibly of even greater concern is the potential degradation of the natural immune system itself from antibody dependent enhancement and the phenomenon of increased viral infections caused by original antigenic sin.
Does reality shows harms outweighing the benefits?
See also - Antibody-dependent enhancement and SARS-CoV-2 vaccines and therapies; antibodies could exacerbate COVID-19 through antibody-dependent enhancement (ADE). Previous respiratory syncytial virus and dengue virus vaccine studies revealed human clinical safety risks related to ADE, resulting in failed vaccine trials.
You would have thought that of all people, policy makers would be aware of the old saying to be aware of lies, damn lies and statistics. May be they are, but we are seeing little evidence of it and this is especially true for children. The official UK immunological advisory group (JCVI) warned against vaccinating children as the harms could outweigh any benefit. Now, the latest reports appear to be confirming this fact. The risks of otherwise healthy under 18 dying of Covid are less than the risk of dying from Flu, which is also very small. The actions have been utterly disproportionate to the risks. The indications are that lockdowns and jabs will end up killing far more younger people than Covid. As reported by the Daily Telegraph following a publication in the journal Nature, "Covid killed just six healthy children during the pandemic, while lockdowns have fuelled a timebomb of health disorders among the young".
There are increasing numbers of reports voicing concern over how bias and other 'confounders' are impacting on the vaccine effectiveness data, such as - The Flaw at the Heart of the UKHSA’s Vaccine Effectiveness Study. These concerns should be taken very seriously as they have a profound impact on the risk / benefit estimates - and especially how they compare even within relatively short spaces of time.
Dr Maryanne Demasi states, "The way authorities have communicated risk to the public, is likely to have misled and distorted the public’s perception of the vaccine’s benefit and underplayed the harms. This, in essence, is a violation of the ethical and legal obligations of informed consent".
Is mis-categorisation of vaccine status masking the spike in deaths?
Professor Norman Fenton, Professor of Risk Information Management at Queen Mary University of London having conducted detailed analysis of the data reports that there is "no evidence of vaccine efficacy based on all-cause mortality". He points out that the data suggests systemic mis-categorisation of vaccine status and uncertain effectiveness of COVID-19 vaccination. He also points out the spike in deaths immediately following vaccinations, which the mis-categorisation caused by the 14 days rule means these vaccinated patients are labelled inappropriately as 'unvaccinated'.
Professor Fenton's presentation to The World Council for General Assembly. He concludes as follows:
1. Vaccine effectiveness studies are generally flawed.
2. The anomalies in the ONS report most easily explained by misclassification of some unvaccinated deaths as vaccinated.
3. After adjusting it appears that shortly after vaccination people may be exposed to an increased mortality risk.
4. The ONS data is both unreliable and misleading.
5. The ONS data provide no reliable evidence that the vaccines reduce all-cause mortality.


